Offering a better way
Urinary disorders, incontinence or retention affect millions of people all over the world. In the USA, 14 percent of all men suffer from urinary incontinence and 51 percent of all women, who are affected more than men due to their anatomy.* Urinary disorders can have many different causes, can develop in varying degrees of severity, and occur in both acute and chronic forms. However, modern medicine offers remedies for even the most severe cases.
Ref: * Markland, A.D., Richert, H.E., Fwu, C.-W., Eggers, P., & Kusek, J.W. (2011): Prevalence and trends of urinary incontinence in adults in the United States, 2001 to 2008. The Journal of Urology, 186 (2): 589-593. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3197263/ (viewed on 01 March 2018)
Three methods of bladder emptying
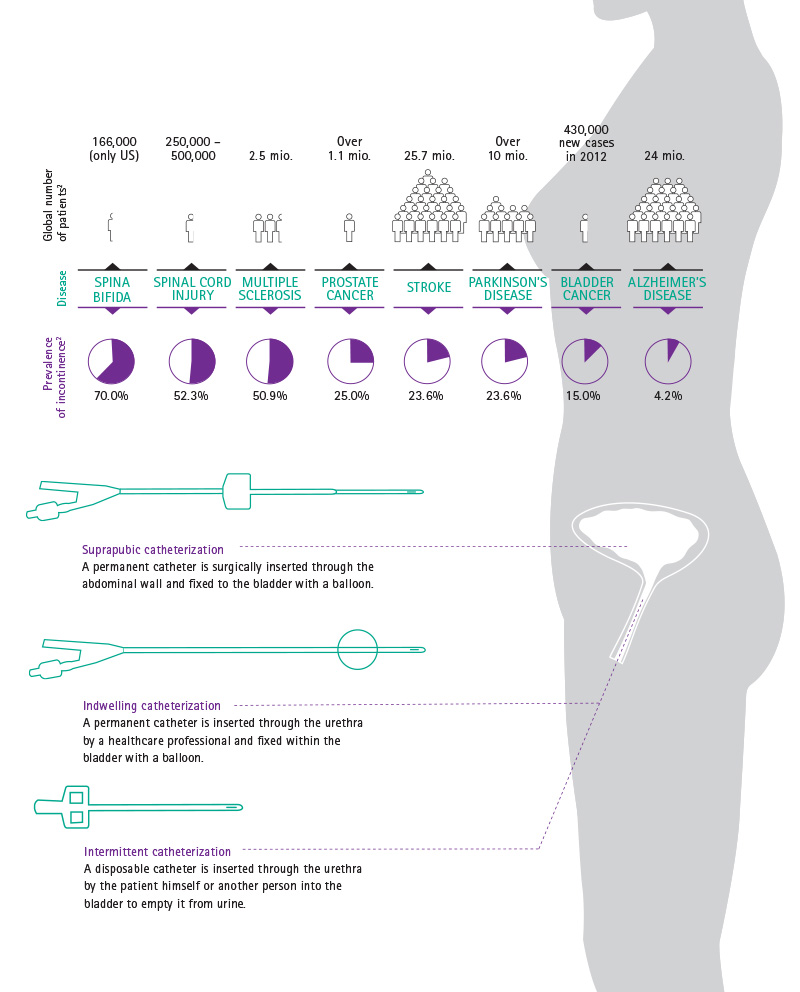
In many patients, the neurologic control of the sphincter and pelvic floor muscles is impaired or even non-existent. The reasons for this can be spinal cord injury, multiple sclerosis, spina bifida, prostate or bladder cancer, but also stroke or Alzheimer's disease. The consequences: the urine either remains in the bladder or is emptied uncontrollably – in either case, a urinary catheter is necessary.
The most common is the so-called intermittent catheterization (IC) technique with a disposable catheter. Used four to six times a day, a thin tube with drainage holes, called catheter, is inserted through the urethra to the bladder to empty it from urine. It is removed immediately after drainage has ceased. It could be performed by healthcare professionals or the patient himself (ISC - intermittent self catheterization).
The second technique is with the indwelling Foley catheter. This type of catheter is inserted through the urethra and fixed within the bladder with the balloon positioned on the top of the catheter. It should be connected to a urine bag for continuous urine collection. This catheter can remain in place for days or weeks. However, permanent catheters are associated with a higher risk of urinary tract infection and should be used only when no other bladder management method is available.
In the third catheterization method, the suprapubic method, the catheter is inserted through the abdominal wall instead of the urethra. This method is performed when the urethra is pathologically narrowed, blocked, or after surgical interventions, in particular within a posttraumatic context.
B. Braun solutions for all three methods

For the intermittent method, we offer our Actreen® catheter product line. We also offer the set version (preconnected catheter and urine bag) specifically for patients that want to stay active and transport the set conveniently in their daily life. A no-touch- system enables safe insertion of the catheter without the user having to touch the catheter itself. The intermittent technique shows great advantages in terms of reduction of urinary tract infections compared to a permanent catheter. It improves the life of patients suffering from body shame. Those patients, who can practice self-catheterization with the help of solutions such as Actreen®, will no longer have to cope with embarrassment and thus can enjoy an active social life.
The Urimed® Cath combined with the Uro-Tainer®, the urological flushing solution, has proven successful for use as a permanent catheter management reducing blockage and incrustations.

The first B. Braun Cystofix® range was launched more than 40 years ago. When suprapubic catheters are used, it is particularly important to insert them as carefully as possible through the abdominal wall. Our last innovation, the Cystofix® SG system enables this, with cannulae that have a diameter of only 1.3 millimeters.